Deciding my Road
When I was a kid, I always dreamed of winning the Nobel Prize by finding the cure for AIDS. I wanted to do research, indulge myself in the world of viruses and finding this elusive cure for a disease that was an endemic before I was even born. I wanted to be like Gertrude Elion who won the Nobel Prize for Medicine by finding the first anti-retroviral drug Acyclovir.
Then I did ONE year of research and HATED it! Oh my !@#$%$^%^&(*!! Who can stay still in a bloody lab, hunched over ELISA plates for the rest of their lives?! Oh, not me. I am so not going to waste my time in labs.
But I still want to win the Nobel Prize or at least leave my name in the future medical books, and what better way to do it than to discover some new surgical techniques or new signs.
My new idol is
Dr. Augusta Marie Dejerine-Klumpke. Yup, she found the
Klumpke's Palsy. Now who is Augusta Marie Klumpke? She was an American who was brought up in Germany, educated in Switzerland, before going to Paris to study medicine. In her third year as a medical student, she described a paralysis of all the intrinsic muscles of the arms and true claw hand paralysis and this is due to radiculopathy of C8 and T1. For that thesis, she won several medical science award in the field of anatomy.
 This is the exact picture found in Dr. JPJ's brachial plexus notes.
This is the exact picture found in Dr. JPJ's brachial plexus notes.She became the first female intern in a Paris hospital and married her professor, Jules Dejerine. Both of them became famed neurologist and neuroanatomist, and Augusta Klumpke became the anonymous collaborator and illustrator for most of her husband's writings and books.
The reason she is my current idol is because like her, I am in my 3rd year of medical school and she inspires me by the fact that even a student can achieve great things. And even better is the fact that she was into neurology as well.
A MBBS degree means I can either choose to be a physician or a surgeon. So for the life of me, I will never ever choose physician. I work better with my hands than my head, so I have always wanted to be a surgeon. I always tell myself, if I want to do something, might as well aim for the most challenging one and reach the top, that way I really stand tall and say I did it. So I have always opted for what I thought is the most difficult field of medicine:
neurosurgery. Yes, playing with nerves of the brain and the spinal cord, joining broken nerves together.
And the sound of a high speed cranial pneumatic drill... salivate.
But what about orthopaedics? This field of surgery gives me a bigger margin for error, after all, bones are bigger than nerves. And have you seen the chainsaws!! Walking into a ortho OT is like walking into a hardware store.
Bbbbrrrzzzzz... eeeehhhhhhggg (chainsaw sound).
I always prefered open surgery, where the chest is flung open, the ribs sawn and spread apart; or the skull taken off to reveal the entire brain; or a huge gaping hole in the abdomen where you can see the yellow fat and juicy organs glistening with blood. To be able to twirl a scapel stylishly and cut right into the body, like how a butcher twirls his chopper before butchering a pig, and to feel the blood splatter, that is what I call a surgery.
But things are turning away from those huge ass surgeries now. Doctors are opting for surgeries that do not have so much scarring or trauma. And this is done by making small incisions and having cameras within the body and long long instruments to do the job inside the body while we control from outside.
This is where we come to the topic of endoscopy. People usually thinks that endoscopes are just that tube that you insert the mouth to look into at the patient's oesophagus, stomach and duodenum. But endoscopes are scopes to look into the human body, and endoscopy includes:
The gastrointestinal tract (GI tract):* esophagogastroduodenoscopy - commonly called endoscopy because this is the most endoscopy done.
* small intestine
* colonoscopy
* proctosigmoidoscopy
* Endoscopic retrograde cholangiopancreatography (ERCP)
* Duodenoscope-assisted cholangiopancreatoscopy
* Intraoperative cholangioscopy
The respiratory tract* Rhinoscopy
* Bronchoscopy
The urinary tract* Cystoscopy
The female reproductive system* Colposcopy
* Hysteroscopy
* Falloscopy
Through a small incision:* Laparoscopy
* Arthroscopy
* Thoracoscopy
* Mediastinoscopy
And of course with the endoscopes, we have the endoscopic surgeries, something that I am looking for. The most common endoscopic surgeries done would be the laparoscopic surgeries. And the one I was interested in was the endoscopic brain surgeries. I am an avid video-gamer, I prize the manual dexterity of my hands. I have not touched a endoscopic surgical instrument before, but I believe that it is going to be one tool I can easily master
(let's not talk so fast first).
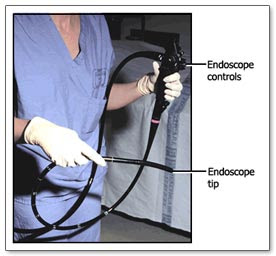
And then I saw the endoscope, not the surgical instruments but the plain old scope, used by physicians and not surgeons.
This piece of equipment is simple, consisting of a tube linked to the controller which is so super cool. You hold the controller in your left hand and the shaft in your right, meaning you must be very ambidextrous. Both hands got to think separately. Ok, I play PS2, I'm used to have two hands doing two different things, I play the piano, again both hands play different notes all the time.
I have seen an endoscopy before, and I was never attracted to it until I saw
Dr. Johannes Wittmann (Gastrointestinial Consultant) uses it. He made using an endoscope looked like a dance, his right hand worked in perfect coordination with his left. Never mind that he is left handed, it doesn't really help that he is cute and nice as well.
Dr. Johannes Wittmann graduated from UQ and then served in the public system for 7 years before going to London (University College Hospital) for his specialty. He is a physician with a Fellow in Pancreatobiliary Medicine and he is like me, he slants towards the procedural side of medicine. He has special interest in ERCP and is the only public doctor in the hospital that can perform an interventional ERCP.
I think I need to rein in my obsession with untouchable guys, but it really does not help with him being cuter than the other consultants I have in the hospital. Granted that I have some consultants who are extremely young (29 years old being the youngest I have met), and the Respi Consultant is pretty hype with all his bling bling, no one comes close to being as adorable as Dr. Wittmann. His cheeks are always red and his ears are so cute and small, like a chipmunk. And his startling grey blue eyes made me realise that it is very difficult to perform a consensual and accomodation reflex on Asians brown eyes. And that casual nonchalant stance he has as he leans against the wall or counter, and that wide smile.

vs

Guess how old is the good doctor?
And I think I have fallen in love with the name 'Johannes'. Seems so sophiscated and mature.
"As a doctor, you need to have maturity and sophistication to grab your time back from the examiners." - Dr. J. Wittmann, on answering viva questions.
So coming back to endoscopy.
I first observed Dr. Wittmann perform a simple esophagogastroduodenoscopy when I popped into his consultation room and he happened to be carting a patient away for the procedure. So I and Rajinder decided to go along. And then I saw him used the endoscope with such dexterity that I could only stare at his big hands as he manipulated the tool. I have seen other doctors perform an endoscopy, they fumbled with the controllers with both their hands, and yet Dr. Wittmann just inserted the shaft with his right, his left thumb twirling the knobs, his other remaining fingers pressing the buttons for water, suction, air and image shot.
I know I was supposed to pay attention on the screen but his hands were just fascinating and his voice just so soothing...
Then there was the time the nurses and registrars were talking about him doing a colonoscopy on this young patient who was having Crohn's disease and was in pain and distress. Dr. Wittmann performed the colonoscopy with minimal sedation, and he was talking all the while with the patient, and he even reached the terminal ileum. And he did it in a record time.
"When I do the procedure, it is just too stimulating." - Dr. Johannes Wittmann, commenting on his colonoscopy technique when a registrar commented that her patient was still sound asleep.
And his next procedure was the one that sealed the deal - the ERCP.
JW: Ward round's over, you can go off with your colleagues for lunch.Me: No, I want to watch the ERCP.JW: Oh, then go get changed.There I was, the
rude medical student who was already dismissed but insistent in joining the ride. He was nice enough to take me to the changing room to get my scrubs, he patiently taught me the route to the OT and even instructed old stupid me on how to wear the lead vest and skirt because I put it on upside down.
So I lingered around, a
useless medical student being a nuisance in the tightly packed operating theater. And then he started.
ERCP is a procedure of inserted an endoscope into the duodenum and from the opening of the common pancreatic duct, insert a catheter into the ampulla and up into the biliary duct to observe the biliary tracts by injecting a dye and Xray-ing the area. And Dr. Wittmann did it which such flair and elegance that I was enchanted. He placed the shaft into the mouth of the patient. I looked away for a moment to get his phone out of his pocket and when I looked up, the camera was already in the duodenum.
I mean, what the hell? So freaking fast!
On a side note, girls should always wear something over their underwear before putting on the scrubs pants. If Dr. Wittmann had done that, I would not have known that he is an underwear guy, black underwear in fact. Haha.Then the scope was in the duodenum and he pointed to the screen.
"So what do you see, Elena?"And I went...
"Huh? Are you in the duodenum?" (Wow, Elena, smart...)
There was this tiny flower thingy on the wall of the duodenum that seemed to shrink and open like an anemone. And that is the opening to the pancreatobiliary tract.
And now comes the difficult part, blind cannulation of the ducts. Because the scope is too big to enter the ampulla, a cannula is inserted into the ducts, and this is done blindly with some occassional help from the X-Ray.
JW: Screen!And the Xray will be on for less than 20 seconds.
JW: Oops, wrong duct.And then the Xray goes off and he will work a while before calling Screen again to show that he is in the right duct and ready to proceed.
He now has to handle three things: the
controller, the
shaft, and the
catheter, and he made it look so freaking easy. He even had the time to tell me what was going on, calling for extra screens to show some stuff that I could not understand.
JW: Screen. Elena, can you see that I am just before the cystic duct?Me: Huh? (Words going through my mind:
What the fuck is the cystic duct)
Xray turns off.
Me: So why can't you go into the cystic duct? (Trying to assume that I know what is the cystic duct)
JW: I'm inserting the dye now. Screen. See, you can see that it is tortuous and blocked.Me: Ahh... (Only understand abit).
And then he backtracks towards the hepatic ducts without any help of the Xray. The rest of the procedure involves ballooning and removing gallstones. There was also a bit of burning (sphinterectomy) and the smoke caused the sleeping patient to fart.
But most of my attention was on Dr. Wittmann. His left hand never left the controller, it twitches the dials to direct the flow of the catheter, his arm flexes back and forth to adjust the scope.
Throughout this whole process, there was a new nurse who was just learning how to assist in an endoscopy. She was fumbling with everything, and Dr. Wittmann just turned and give her this oh-so-boyish smile and said,
"Calm down, I will not bite." And he taught her how to be a nurse. I have seen other surgeons who would have snapped at the nurse.
After the whole thing, he sat me down as he prepared the report and talked me through what he had done and what he would have done if not for risk factors, bla bla bla. Most things just flew over my head because it is a subspecialty knowledge and the headiness of being there just listening to him talk, haha. Have I told you he has a very soothing voice?
Watching this procedure made me realise, if using endoscopic surgical instruments is like playing PS2, using the endoscope is like playing Wii.
 vs
vs 
 vs
vs 
So now there are two
'gaming instruments' out there waiting for me to play. And with
NOTES coming up, life is gonna be good for a gamer eh? And do not forget the
Lindbergh Operation where the surgeon operates a robotic arm, and when the first micro robot enters the body to perform a microsurgery, I will be the first to be behind those controllers.
I just can't wait to start neurosurgery and start playing with all these tools. But the problem is I don't think OZ have endoscopic brain surgeries or brain endoscopy. Well, we will just have to wait till I start my surgical rotation. Can't wait!!!
But being with Dr. Wittmann had opened my eyes to the world of procedures done in the Gastroenterology Unit. The endoscopes, the laparoscopes, you get to play with much more 'gaming instruments' than in the brain.
And remember what I was saying about aiming for the best?
The surgery claimed to be the toughest by John Hopkin's Chief of Surgery is the
Whipple's procedure also known as pancreaticoduodenectomy. Reasons for it being tough:
1. The pancreas is behind the stomach, duodenum, bile duct and gallbladder.
2. There are lots of large blood vessels in the area.
3. The pancreas is friable and damn tough to stitch.
4. Pancreatic enzymes destroys flesh like nobody's business.
5. You have to reconstruct the pancreas and the gastrointestinal tract.
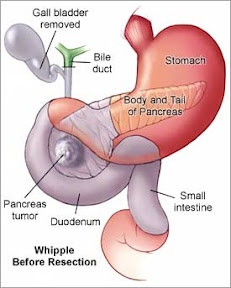
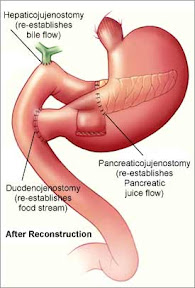
Before and after Whipple's.
The
Ivor-Lewis procedure (oesophagectomy) has a mortality rate that equals heart PLUS lung transplant.
1. You split open the rib cage.
2. You deflate the left lung.
3. You go around the heart and pull out the oesophagus.
4. You resect the part of oesophagus.
5. You pull part of the stomach through the diaphragm.
6. You sew the two ends together.
7. Inflate the lung and you are done.
But then again it is very difficult to say such things as each field has its own medals of honour and their own equivalent of the Whipple's or Ivor-lewis.
The
nerve-sparing radical prostatectomy is done by urologist and involves resecting the entire prostate without damaging the nerves and sewing the bladder back to the urethra.
The staples (bone in the ear) replacement of the ENT team is also as difficult because you are working in such a small area.
The cardiac surgeons have the
Batista procedure (left heart reduction) and the Paed cardiac surgeons have to squeeze their huge hands into that tiny walnut size heart.
So what about my favourite field, NEUROSURGERY? John Hopkin's Chief of Paediatric Neurosurgery was 33 when he became Chief and he majors in
hemispherectomy (removal of one half of the brain) in children and he was famous for separating a pair of siamese twins joined at the head! And imagine trying to untie some baby's spinal cord which is so tiny.
So until I have done my surgical rotation, this is going to be tough to decide. But I kinda have it planned out. I have two choices each for my Surgical and Medical Specialties, so I'll most probably be doing:
Medical Specialty:
Neurology, GastroenterologySurgical Specialty:
Neurosurgery, Orthopaedics"Pass Medicine rotation first only talk." - Richard Lee.
But let's see what my
aptitude test says:
1 radiology
2 urology
3 nuclear med
4 neurosurgery
5 gastroenterology
6 allergy & immunology
7 pulmonology
8 pathology
9 plastic surgery
10 aerospace med
11 neurology
12 anesthesiology
13 emergency med
14 dermatology
15 endocrinology
16 cardiology
17 ophthalmology
18 otolaryngology
19 thoracic surgery
20 infectious disease
21 colon & rectal surgery
22 preventive med
23 orthopaedic surgery
24 pediatrics
25 general surgery
26 radiation oncology
27 nephrology
28 occupational med
29 psychiatry
30 obstetrics/gynecology
31 general internal med
32 rheumatology
33 hematology
34 physical med & rehabilitation
35 med oncology
36 family practice
Hmmm... the first three is wrong, but 4 and 5 reflects my vision. Maybe this is a sign. haha. And as you can see with the last few ranks, I hate taking care of people, so maybe radiology suits me in the way that I do not have to deal with any patients at all! But I would be nothing but a technician... OMG, downgraded!
(No offense to the techies. Without you guys, the hospitals will never be able to function, but I just don't see myself doing technical stuff.)And if I do take the Gastroenterology Specialty, let it be at my current hospital and my consultant be Dr. Johannes Wittmann. I am so going to learn all my endoscopic skills from him. Not only he is a great doctor, he is a great teacher as well. I just hope I don't get on his bad side - he was seen reprimanding a group of 2nd years and they all looked like whipped puppies with tails between their legs.
But I just find him so very fascinating. And oh ya, I barely reach up to his chest. And I realised that my one hand can not even reach the dials of the controller. They really do need to make a smaller version controller.
Cyrus! My life regaineth its meaning!
- Frog, Chrono Trigger






